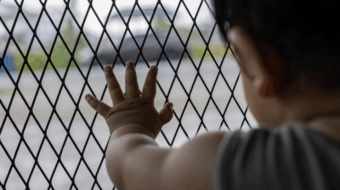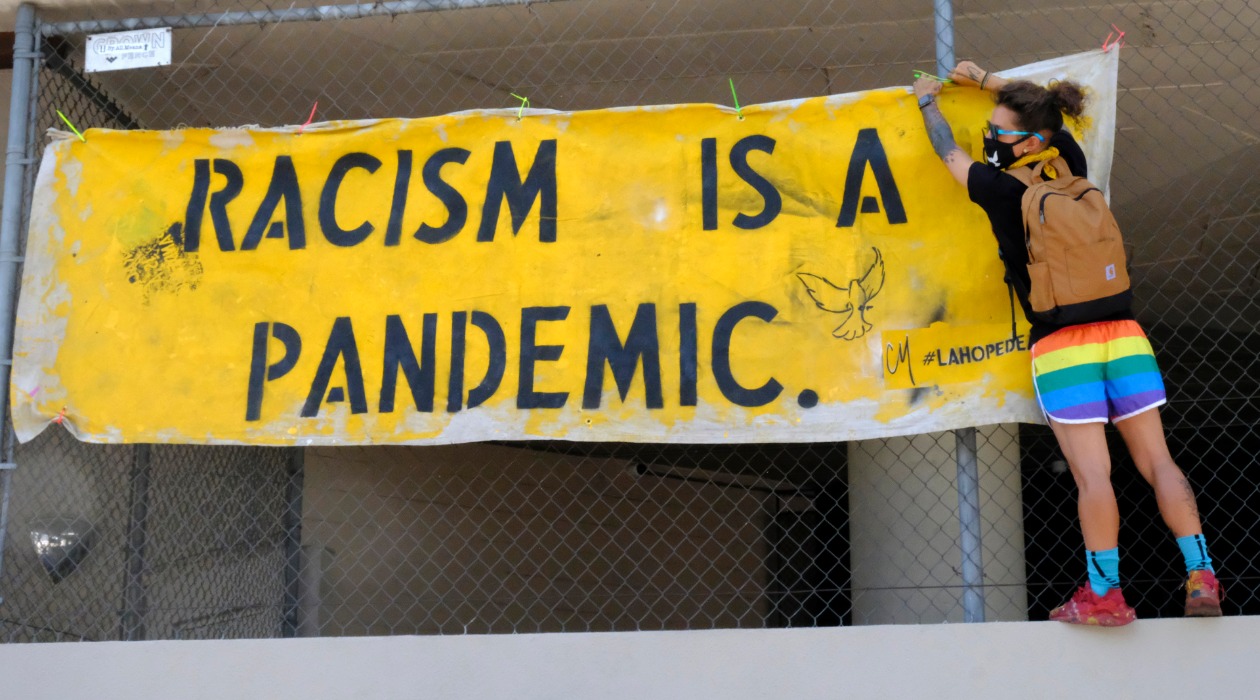
ATLANTA—The yawning gaps in health care among different U.S. racial groups, exposed and accelerated by the coronavirus plague, have led the federal Centers for Disease Control to officially declare racism “a serious public health threat.”
But because of the nation’s concentration on battling the virus, which has killed more than 928,000 people since it was officially proclaimed almost two years ago, is so great, CDC’s decision has been virtually overlooked.

It shouldn’t be. As a result of systemic problems affecting communities of color—including bad housing, more-dangerous jobs, and outright discrimination, the U.S. has had “a known, but often unaddressed, epidemic impacting public health: Racism,” CDC Director Rochelle Walensky, MD, said when she unveiled the agency’s decision last year.
How overlooked has racism as a public health threat been? An internet check of who publicized the story last April showed it ran in some specialized journals, plus Rolling Stone and three major mainstream media: National Public Radio, the website for what once was the U.S. News and World Report, and Fox, which played it straight. Not The New York Times. Not The Washington Post. Not other broadcast networks. They were all concentrating on the virus.
Nevertheless, Walensky discussed the health impact of racism, and her agency is following it up with more programs, studies, and outreach. It also sought, and got, more money from Congress for the project.
“The impact of COVID-19 is felt, most severely, in communities of color—communities that have experienced disproportionate case counts and deaths, and where the social impact of the pandemic has been most extreme,” Walensky said then.
Though Walensky didn’t include any numbers in her speech, the American Public Health Association, in a resolution six months later, did. But since the start of this year, it’s identified another problem that could make matters worse: Resistance to public health moves.
“Black Americans have historically and continually faced systemic ‘racism, segregation, and economic disinvestment’ throughout American history, significantly contributing to disproportionate levels of poverty and chronic disease relative to non-Black Americans,” APHA’s heavily footnoted first resolution says.
“As of July 2021, Black Americans were 2.8 times more likely to be hospitalized and two times more likely to die from COVID-19 than White Americans…Hispanic or Latinx persons were 1.9 times more likely than White Americans to contract COVID-19, 2.8 times more likely to be hospitalized, and 2.3 times more likely to die.”
But the racial gap which led to CDC’S decision came not solely from the virus’s slam of people of color.
Instead, the virus exposed longstanding racism permeating not just health care, and highlighted “social determinants of health” that racism affected.
Walensky asked for, and Congress agreed, to invest more money in research on racism as a public health threat: $74 million for the year that ends Sept. 30 for the main investigation and outreach program, called REACH, on racism as a public health threat. That’s $10 million more than the year before.
REACH stands for Racial and Ethnic Approaches to Community Health. A CDC factsheet webpage describes it as “aimed at reducing racial and ethnic disparities in health.” State and local applicants who get Reach grants are supposed to “bring together members of the community to establish community-based programs and culturally tailored interventions serving African Americans, American Indians, Hispanics/Latinos, Asian Americans, Alaska natives, and Pacific Islanders.”
Outreach to communities of color got four times as much, or $300 million, CDC said. That’s going to be used to reach those groups in a variety of ways: To “strengthen the work of community health workers, nationwide, in their efforts to prevent and control Covid-19 among high risk populations and communities hardest hit by the epidemic” and to communicate the risk to leaders of those communities, such as Black church pastors.
Then there’s the worksite problem. Jobs millions of workers of color hold only make a bad situation worse, APHA said.

In information that is not news for those communities, APHA reported “most U.S. workers cannot work from home, and those who work in proximity to others tend to have lower incomes, have less access to health insurance, and lack paid sick leave.
“A lack of paid time off may promote attendance at work despite sickness or recent illness exposure. These working conditions are also risk factors for preexisting conditions that increase COVID-19 severity. Black, American Indian and Alaska Native, and Hispanic and Latinx workers are more likely to have jobs with lower incomes, to use public transportation to commute, and to live in densely populated areas, and they are less likely to have health insurance.” All increase exposure to COVID-19.
And all are systemic conditions based on race which Walensky was discussing, even if not in detail.
“Workers of color also have lower job control and greater job insecurity,” APHA said. “A study of poultry workers showed physical proximity to other workers and shared equipment can facilitate” coronavirus “transmission at work,” a point unions, particularly National Nurses United and the United Food and Commercial Workers, have repeatedly made.
“Other work settings with significant outbreaks of COVID-19 include correctional facilities, nursing homes and long-term care facilities, homeless shelters, and manufacturing plants. Because work data are not being systematically collected and reported for people with infections, information about worksite exposures is largely limited to news reports,” APHA added.
But the battle against the coronavirus has produced a backlash “of mistrust and disregard for public health science, public health measures, and public health officials,” APHA warns in an understatement.
“The ability to determine whether public health measures are needed to address issues that pose significant risks to the health and well-being of communities has been dramatically limited or reassigned to elected officials” who don’t know, or want to know, science or public health.
The officials “and others” contradict or ignore public health officials and workers and harass or threaten them and their families. Politicians fire some public health workers, while others drop out or retire early.
That leaves people interested in protecting public health—much less battling racism as a public health threat—with “an inability to protect the communities they have served, exhaustion, and a bleak forward-looking picture,” APHA says.
CONTRIBUTOR