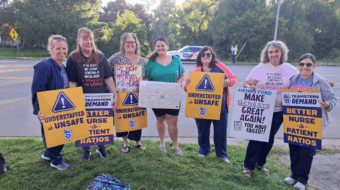
TORONTO—Ontario’s emergency medical system is in an escalating crisis, with no plan from government leaders to do much of anything. While politicians pass the buck, outright lie, or refuse to admit there’s a problem at all, patients and frontline workers—nurses, paramedics, doctors, and other professionals—are watching our health infrastructure fail the sick and vulnerable more and more every day.
Paramedic services are reporting a terrifying increase in “code zeroes”—instances when a service has zero available ambulances to respond to calls within its response areas. There are multiple reports of “out of town” ambulances traveling for over an hour with their lights and sirens on, to high acuity code zero 911 calls. It’s hard to overstate the severity and absurdity of what’s happening.
It’s like if you lived in Toronto, hired a babysitter in Niagara Falls, gave them the receiving end of the baby monitor, and told them to “drive as fast as you can” when your child starts crying.
Wait times for an ambulance and ER wait times are related and are affected by three general factors: available capacity in hospitals at large, available capacity in the ER, and available capacity of ambulances. The capacity issues at each stage affect the preceding one.
For example, the lack of beds on hospital floors prevents admitted patients from moving out of the ER, which in turn keeps beds in the ER occupied despite the fact that those patients cannot be treated effectively there. Full ER occupancy means that patients brought in by ambulance don’t have a bed because there isn’t nursing capacity to monitor them.
This results in “offload delay”—in which paramedics are forced to stay in hospital for up to 10 hours or more to monitor these patients themselves—which in turn takes ambulances off the road and exacerbates the staffing crisis of already underfunded and poorly staffed municipal paramedic services.
The idea that an emergency service would have zero surge capacity is ridiculous. Firefighters never run out of resources, and paramedic services should be staffed to respond to large scale crises. Yet, we can’t even respond to routine call volumes.
It’s easy to conclude that the code zero ambulance crisis is simply an outgrowth of the hospital crisis, but this is an oversimplification. Certainly, the nursing shortage—which is related to decades of systematic reductions in per capita healthcare funding and exacerbated by government wage caps—leads to offload delay and resultant ambulance shortages.
Indeed, this is the party line for almost all municipal services, especially in Toronto, and one that is parroted non-stop by the Ontario Paramedic Association (a management organization which does not represent workers).
But this narrative is only a small part of the truth, one that is convenient for the cadre of supervisors and managers who refuse to take any responsibility for the most pressing issue: not being able to respond in time to save a life. Why are these “leaders” paid to captain such a critical public service onto the rocks?
Paramedic services have an extraordinarily high attrition rate, with most services in Ontario competing over an ever-decreasing pool of qualified applicants. The reasons for this include long work hours and grueling shift work, cuts to real wages, lack of breaks, forced overtime, compassion fatigue, PTSD, low morale, and a constant frustration that the system isn’t helping the majority of our patients.
This creates two problems: not enough paramedics to work in the first place, and many medics unable to work due to stress, exhaustion, or illness.
While management mercilessly squeezes medics, they rely on our continued empathy, compassion, and professionalism to keep things running—ask any nurse and they’ll tell you that they’d strike in a heartbeat, but their patients come first. It’s also no secret that capitalism in general undervalues all caregiving work, be it parenting, support work, nursing, mental health, paramedicine, etc.
Canadians are among the highest per capita users of emergency medical systems worldwide, yet the country has an underfunded infrastructure. As the population ages, poverty increases, and healthcare funding is reduced, paramedic services are also dealing with rapidly increasing call volumes.
The World Health Organization says that “social determinants can be more important than healthcare or lifestyle choices in influencing health.” In emergency services, we have more patients simply because people are poorer and, as a result, are disproportionately suffering from diseases like diabetes and heart disease, or “social issues” like mental health, drug and alcohol use, and homelessness.
Poverty is endemic to capitalism, which requires it to keep the working class desperate enough to accept low wages and to hinder mass organization. But poverty also generates a subset of the population deemed to be worth nothing at all, so we see the steady erosion of social services to that group. As a result, increasing numbers of people become less able to lead healthy lives and find their way into emergency healthcare.
All of these issues are exacerbated by privatization. Private long-term care facilities have far worse resident health outcomes than public facilities, and they frequently do not staff the health professionals to treat the complex medical needs of their residents. Instead, they offload that care and the costs onto the emergency system.
Meanwhile, provincial governments like Ontario’s are steadily privatizing healthcare. In paramedicine, there’s been talk of moving back to private models (which already exist through companies like helicopter medical evacuation service Ornge), and this opens the door to a U.S.-style system which deskills medics to make them more expendable, jeopardizing patient care in the process.
An underappreciated aspect of emergency medicine, paramedicine specifically, is how it is affected by municipalities’ obsession with liability. Local bureaucrats tend to care less for actual patient outcomes than about whether or not they’ll suffer any consequences related to the service they’re providing. Consequently, the system compels paramedics to convince patients, no matter their condition, to be transported to hospital rather than provide those patients with their options so that they can make informed choices about their care.
This obsession with liability infects all areas of healthcare and creates a system which excessively triages many people into ER, despite that not being the most appropriate place for them to seek care.
This unearths a deeper contradiction related to the social determinants of health: Why is it that the state feels obligated to provide emergency care to people when they call 911, but not to ameliorate the risk factors associated with calling 911 in the first place? Why is it appropriate to allow people to languish in poverty until they become so desperately ill, and lack any other resources, that they have no choice but to call 911, one of the few social services left which can be accessed immediately? Why does the state accept that people who are chronically ill due to their social circumstances deserve care in their most desperate moments, but they don’t deserve to have better social circumstances?
Of course, the problem isn’t lack of resources, but the fact that capitalism is functionally incapable of such a response.
As with all op-eds published by People’s World, this article reflects the opinions of its author. This article originally appeared in People’s Voice.
CONTRIBUTOR