


After suffering a medical catastrophe—with the bills to match—I am lucky to be both alive and solvent. I have long been an advocate for the housing needs of the underserved population of Long Island. My recent personal experience has, however, inspired me to think beyond the housing crisis and consider the inextricably related issues of cost and access to medical care in the United States. Change is necessary for the wealthiest country in the world to match that status with being the healthiest place for all of its citizens, without regard to income.
For several years, I was a tenant organizer in Hempstead and other vulnerable areas on Long Island. While canvassing, I learned that many people I visited live in unimaginably sub-standard housing. Even worse, many suffered from health maladies related to their living conditions. I considered myself extremely lucky, not only to live in my own home, but also to be in good health.
The latter good fortune, however, took a dramatic turn in April of this year when I underwent my own health crisis. What started as an unusually high fever progressed quickly to the complete loss of control of my arms and legs. I was, frankly, near to death, or to a life-long struggle with quadriplegia. After diagnosis of a spinal infection, I was rushed to emergency surgery. I was to be hospitalized twice more, and was bedridden for months, reliant completely on others for the most basic of my needs.
My life was saved, and my outlook is good. While I will not bore readers with the specifics of my therapy, I am happy to report that I am back on my feet, physically and emotionally.
What saved my life, and quite literally, my limbs, was the fact that I was able to afford around-the-clock assistance from two gentlemen who, along with my wife, cared for my every need. I was also in a position to afford therapeutic care from a variety of health care providers. The cost of this care was well beyond what medical insurance or health care “entitlement” programs would have provided. Simply stated, the cost of my care was astronomical.
Reflecting on my situation, I find myself thinking of the people who I came in contact with as part of my housing organizational efforts. Where would they be in a similar situation? Absent the level of care that I was able to access, it is likely that my outcome would not have been the same. Resources available to me are simply not available to those without the means to pay. I began to research and think about the state of health care in this country and to consider how to help ensure that everyone in this rich country is entitled to the same level of care that my privilege allowed me to access.
I first considered Medicare. I am certainly a proponent of Medicare for All. However, the current Medicare system is not nearly extensive enough to take care of the needs of the American population. As a senior, I am entitled to a set level of therapy from the program. The additional therapies that have allowed my recovery have cost me thousands.
The hard truth regarding medical care in the United States is clear: If you have money, you get care; if you don’t, you get the scraps of the medical system.
This reality is grounded in capitalism’s drive to commodification, to make everything into a product to be bought and sold. Housing is a commodity, and so is education and of course health care.
In reviewing research from Commonwealth Health Fund as well as the Pew Research Center in Washington, one of the things that surprised me was that among industrialized nations, the U.S. is the poorest in terms of health outcomes per dollar spent. This has resulted in a drop in the average life expectancy of American people. Life expectancy and mortality rates for people of color show even more dramatic decreases. Adding gender as a factor reveals even greater disparity. For example, Black women suffer postpartum depression at a much higher rate than other races.
Medicare for All is a salutary proposition, but it becomes meaningless if it is not matched with a robust system for delivery of quality care that truly matches the medical needs of the rich as well as the poor.
One cannot discuss the cost of medical care without also discussing medical debt. Such debt becomes inevitable when people cannot afford basic, never mind catastrophic, medical care. Remember my personal situation? Had I not had the resources of all of my family members to aid in my rehabilitation, I would almost certainly be among the many Americans who go into debt or bankruptcy because of the costs of medical care. I thank God that didn’t occur in my case.
But the average working-class citizen faced with catastrophic health needs is often forced to make choices among feeding and housing their families, or meeting their own medical needs or those of the people they love and care for. This has to stop. The cost of care should not result in a lifetime of financial instability for families.
Beyond financial discrepancies, local access to medical care is another issue that must be addressed. If you live in suburbia or a large city you may have access to high quality medical care. Those who live in rural areas with high rates of unemployment experience a lack of such access. This includes those living in areas where mines, steel mills, or centers of manufacturing have long ago ceased to operate. How sad it is that in this wealthy country, vast segments of our population are still not getting what they need.
Many argue that our government simply cannot afford to pay for the health care needs of all. Medicare is funded through taxes, as is another source of care – Social Security. One of the things that I’ve been concerned with for many years is the cap on the payroll tax, known as the Federal Insurance Contributions Act or “FICA,” a source of government funding for health care.
Once annual income reaches a certain amount (currently approximately $168,000), there is no longer an obligation to pay FICA taxes. We all hear Republicans complaining that Social Security is going to go bankrupt. Well, why is it going to go bankrupt? Because the wealthy are not paying enough into that system. We should abolish the cap on the FICA cap, but that won’t be easy with Trump and a GOP Congress. While there may certainly be other sources of tax income, reform of the FICA cap is certainly something that must be considered.
Mental health care is another area of our health system that needs reform. I have worked in both the mental health system as well as the system that provides care and services for people with developmental disabilities. In both, there are serious problems. An example of a family I have worked with makes this clear. Specifically, I have worked with a single parent of a 21-year-old. He is developmentally disabled and has a mental health diagnosis. For the last year and a half, his single mother has struggled to obtain the proper care for her son.

In New York State we have what’s called the “Front Door.” Families need to go through the front door in order to access Medicaid-provided services – meaning they need go through the processes required for obtaining a proper assessment and official diagnosis before being able to receive Medicaid help for services.
As part of her son’s care, the mom has been unable to secure the necessary psychiatric assessment – simply because she can’t afford it. While she should be able to easily obtain the assessment via Medicaid, there is currently a six-month waiting list for a psychiatric evaluation at a Medicaid clinic. The fact that she cannot get care for her son or get him into a day program has caused her to lose her job. She is currently receiving help through the Department of Social Services, but her situation has put her in a worse position than if she had been able to remain employed.
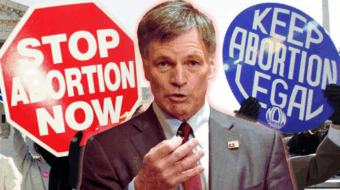
Finally, no commentary on health care in America can ignore the impact of the overturning of Roe v. Wade. Abortion care is health care. Before Roe established the right to abortion health services, only wealthy women had access to such care. Many were able to travel abroad to receive the health care they need.
Roe was the law of the land for 50 years until right-wing Republicans on the Supreme Court decided that abortion, and care for pregnant women generally, would not be tolerated. In the wake of the overturn of Roe we are back to a situation where poor women are once again left to their own, often unsafe, devices to obtain medical care.
Apart from restoring the right to abortion care, we need to provide child care and discretionary family care funding for every family in the United States. Why not give very family $25,000 to make decisions for themselves about their care and needs? How would this be funded? Again, lift the cap on FICA taxes and seek other avenues to tax the ultra-wealthy. Those who work for a living should not be the only ones paying taxes. Working class and poor families need access to high quality day care, and it should be funded by the government.
Even with its shortcomings, we must make Medicare accessible to all from birth to death. When LBJ and Congress set this system up in 1965, they envisioned that by 2005 every person in this country would have medical care through Medicare, regardless of age. Powerful lobbying groups fought against it. Number one were the insurance companies. Number two were doctors. As to the medical profession, changes over the last 50 years in his country have left many people unable to visit private practitioners. Nowadays, the norm is one or two large medical corporations as the only place to receive medical care. Community services and clinics need to be expanded so that all people of different economic backgrounds can receive proper care free of financial obligation.
Those who govern this country need to have their eyes opened as wide as my own recently were. We all need to advocate not only for the end of unequal distribution of wealth but also the equal distribution of quality health care.
As with all op-eds published by People’s World, the views expressed here are those of the author.
We hope you appreciated this article. At People’s World, we believe news and information should be free and accessible to all, but we need your help. Our journalism is free of corporate influence and paywalls because we are totally reader-supported. Only you, our readers and supporters, make this possible. If you enjoy reading People’s World and the stories we bring you, please support our work by donating or becoming a monthly sustainer today. Thank you!
CONTRIBUTOR



MOST POPULAR TODAY

As Iran war rages, Netanyahu builds ‘Greater Israel’ from Palestinian and Lebanese land

Europe refuses war script: Spain’s rebuke exposes limits of U.S.–Israeli escalation in Iran
The other ‘lizard people’: Why the Epstein files are shattering global theory

Trump’s Postmaster General says USPS may shut down in a year

The short story of Fred Hampton, assassinated Black Panther leader