NEW YORK—In the process of gaining asylum and transitioning to the United States, immigrants cope with many health-related issues. Post-traumatic stress disorder and major depression, as well as many often indolent (slowly progressing) infectious diseases, are common among the immigrant population. Professional organizations are taking note of these health care needs.
My professional organization, the American Thoracic Society (I am a pulmonologist), has recently published a position paper on the medical needs of migrant and refugee populations. One example is tuberculosis (TBC). Screening methods and preventive therapy have essentially eradicated TBC infection in the United States. TBC is common in impoverished countries and among migrants, however. To date, there are no precise data as to the prevalence of TBC among migrants and no foolproof protocol for their screening. Screening and treatment are obviously important for both the prospective patient and the communities where they will live.
Dangerous environmental conditions (often associated with global warming), stress (associated with persecution and torture), and poverty bring about a host of medical and psychiatric conditions facing migrants.
Medical issues and medical screening both play an important role in the complex asylum process for many migrants. Screening may provide a brief review of the applicant’s personal history with the goal of corroborating his/her history with that previously given by the applicant to others.
Note here that applicants must demonstrate a “well-founded fear” of persecution upon returning home in order to qualify for asylum. Thus, history is important. Physicians are called upon to document evidence of physical torture in asylum proceedings. Physicians present evidence to the court of either physical torture as observed on physical examination or of mental torture observed on a psychiatric interview. Physicians may observe and describe scars as being consistent with scars that may have resulted from the tortures, e.g., knife-slashing, whippings or bondage (with rope or other heavy materials) the applicants have described. In doing so, physicians corroborate the histories given by the applicants.
Medical professionals with expertise in either gynecological or psychiatric examination are often required. Rape is common and requires examination for sexually transmitted diseases. Evidence of blunt trauma in the remote past may occasionally be seen on rectal or vaginal exam. Mental status evaluation is often complicated. People who have undergone emotional trauma are often reluctant and frightened to recall traumatic events. These assessments must be conducted by skilled, experienced interviewers.
To accommodate the needs of asylum applicants, physicians have formed a nonprofit organization, Physicians for Human Rights (PHR). Founded in 1986 and headquartered in New York City, with offices in Boston and Washington, D.C., PHR shared in winning the 1997 Nobel Peace Prize. It makes itself available to asylum applicants and their legal representation. PHR recruits volunteer physicians and provides them appropriate training in preparation for their examination of asylum applicants. PHR then matches applicants with physicians.
I have served as a volunteer PHR physician for more than fifteen years. Given my background as a pulmonologist/internist, my activities have been limited to corroborating history and describing the residuum of wounds suffered during torture. Over these years I have seen applicants from the Caribbean and Central America (Haiti, Mexico, Guatemala), Africa, the Middle East, and the Balkan Peninsula (Congo, Ivory Coast, Mauritania, Niger, Syria, Kosovo), and China as well.
Perhaps the single most interesting applicant I have seen recently was a 34-year-old man born a slave in Mauritania. I interviewed him nine years after he had come to the United States, assisted by the organization SOS Slaves. He had escaped from his slave master and had lived clandestinely for more than a year in Mauritania awaiting passage here. He had been imprisoned more than once and bore many scars attesting to the trauma he had endured at those times. His story here in the United States has been remarkable. He was placed with a family in Brooklyn. He attended a school in Harlem where he learned to speak English flawlessly. By luck, he entered a vocational school where he learned to drive a truck. He is now fully employed as a truck driver, is self-supporting, and pays taxes.
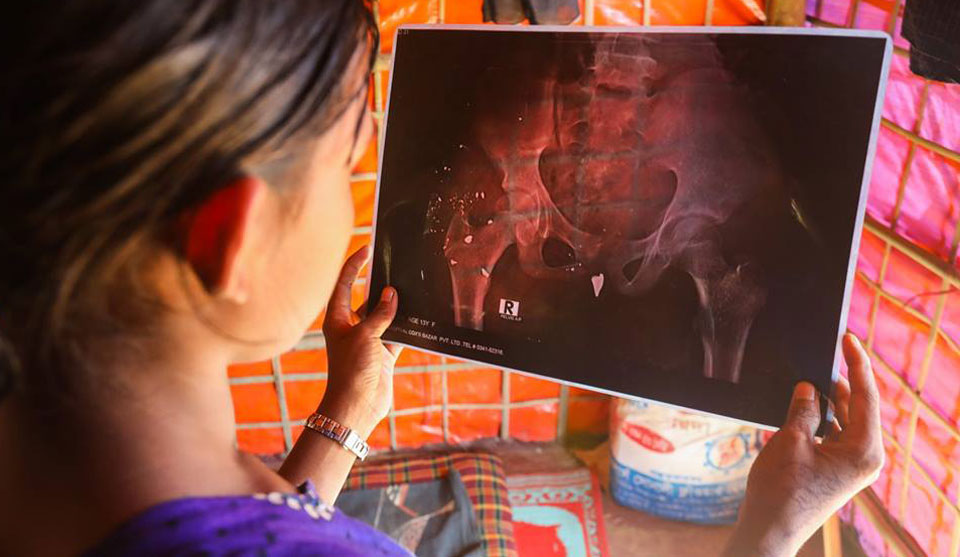
When I examined him, I found and described in my affidavit, many obvious telltale scars. Most striking, he had an obvious linear scar on his right kneecap; the second toes on both of his feet, while mobile, were obviously misshapen. These lesions could likely have resulted from rope burns, incurred while he had his legs bound tightly for many days. His misshapen toes could have resulted from fractures incurred at that time. He had many other circular and linear scars, all of which could have resulted from whippings and knife wounds he has described. My task was to describe some of these lesions simply and clearly in my report. This man was most remarkable in that he was unexpectedly relaxed, articulate, and congenial for a person undergoing this sort of pre-asylum interview. Clearly, he meets the “well-founded fear” criterion. Were he to return to Mauritania, he would have no family or friends to greet him. He would quickly be identified as a runaway slave by authorities and likely face execution.
Eliciting histories from these applicants is an enlightening experience. One young man fleeing Mexico had operated a small retail business (shoe sales) from a pushcart in a public mall in Mexico City. Gang members first extorted money from him and later wanted him to “launder” illegal shipments of cocaine. He refused to comply and in turn was threatened with death.

Another young man from Syria had successfully trained in electronics and had opened his own electronics store. He had an unusual family name, however, a name more commonly associated with Turkish than Syrian background. For this, he was repeatedly threatened and tortured by lackeys of the Assad government.
Many asylum seekers flee harassment for their homosexual identities and acts. These people present a slightly different task for the asylum process in that their cases do not involve political issues. In many unenlightened countries, however, homosexual people are not only ostracized; they are targets of physical violence.
Volunteer work for PHR has provided me with both an eye-opening educational experience and an opportunity to serve others. I am appalled when I read in the press about the “terrorists” and “criminals” converging in caravans on our southern border. But I see in the long run an almost insurmountable problem, a problem we refuse to acknowledge or address. Sectors of our mainstream press portray migration as merely a transient phenomenon perpetuated by “liberals.” In truth, this phenomenon will surely grow, thanks both to global warming, which will shrink arable land, and to the continuing emergence of autocratic governments in underdeveloped nations.
Quite simply, we are not prepared.
CONTRIBUTOR