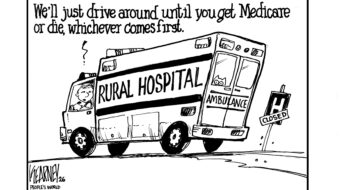
A few weeks ago, a woman gave birth at Hereford Regional Medical Center, a critical access hospital in the Texas Panhandle. Or, rather, the woman gave birth in the parking lot at Hereford Regional Medical Center after driving over an hour to get there, according to Jeff Barnhart, the hospital’s chief executive.
Barnhart said he’s heard it all over the years: patients giving birth at rest stops and in ambulances and in the car on the side of the road. The hospital’s patients come from a 1,600-square-mile area in the Texas Panhandle, and some of them just don’t make it in time.
But now, even patients who do make it to the hospital have another variable to contend with: critical staffing shortages and exploding COVID-19 case counts. There are days when Hereford Regional doesn’t have enough nurses to operate the labor and delivery unit, forcing it to divert patients 50 miles northeast, to Amarillo.
“We give them a medical exam and see if there’s time to get them in an ambulance to another hospital that can take them,” he said. “But sometimes, that baby’s coming and there’s just not time.”
Those patients give birth in the emergency room, an increasingly common occurrence as rural hospitals limit or cease labor and delivery services due to insufficient staffing.
Nationally, the health care system is facing an unprecedented labor shortage as nurses retire, resign, burn out, or leave staff positions for more lucrative travel nursing contracts. Rural hospitals, many of which already operate with a shoestring staff, are especially hard hit.
Declining populations and cuts to Medicaid and Medicare funding have made Texas the national leader in rural hospital closings, with some 26 closures—permanent or temporary—of rural facilities in the last decade. Two-thirds of the state’s 157 rural hospitals are public, which means less flexibility in salary negotiations. Administrators also say it’s often difficult to recruit medical personnel to smaller towns in remote counties.
Struggling to survive, the remaining hospitals in Texas’ rural communities have had to cut back services. And when that happens, labor and delivery is often the first to go.
Only 40% of Texas’ rural hospitals still have a labor and delivery unit, according to the Texas Organization of Rural and Community Hospitals, leaving whole swaths of the state without access to nearby obstetrics care.
“If we’ve got nurses to cover a day, of course, we’re going to try to take care of everything that we can here,” Barnhart said. “But it’s just a scheduling crisis, and whenever we can’t make it work, we just let the hospitals in Amarillo know so they can expect it.”
Cuts to services
Adrian Billings has been delivering babies at Big Bend Regional Medical Center for 15 years, serving patients across a 2,000-square-mile area in West Texas. The hospital delivers about 200 babies a year, he said, with pregnant patients sometimes driving over 100 miles to give birth.
But in recent months, for the first time since he’s worked there, the hospital has limited the hours the labor and delivery unit is open. Over the holidays, the unit shut down entirely for two weeks. For a while, it was only open Monday through Thursday morning.
“When that happens, essentially, it’s a maternity care desert Thursday morning through Monday morning out here,” he said.
He said the hospital tried to schedule inductions during the week as much as possible, but childbirth can be hard to predict. If a patient goes into labor during the off hours, they either give birth in the emergency room or are sent 60 miles away to Fort Stockton.
A spokesperson for Big Bend Regional said in an email that the hospital recently hired additional nurses who will soon allow it to resume full-time maternity care. But many rural hospitals say they simply aren’t able to keep up in today’s ultracompetitive labor market.
“We only have six doctors at our hospital,” said Jennifer Liedtke, the director of the labor and delivery unit at Rolling Plains Memorial Hospital in Sweetwater, about 40 miles west of Abilene. “When you’re talking about a census of 20-plus patients, we’re carrying a full load trying to get everyone seen. … It’s rough.”
Rolling Plains typically tries to have three labor and delivery nurses scheduled for each shift. But recently, Liedtke said the team is scraping by with one nurse and a shift supervisor who can step in as needed. Her nurses often get pulled into other units when there are no deliveries.
“There’s not a patient back there today, so both of [the nurses] are working the COVID unit right now,” she said. “So if we do have a patient come, they have to go shower and change into all new scrubs and stuff before that patient will have to come back.”
Many of the longtime nurses at Rolling Plains retired during the pandemic, Liedtke said, and it’s been difficult to find replacements. On Monday, all five of the hospital’s ICU beds were occupied, according to state health numbers.
“We’re trying to recruit right out of school right now, but a lot of the young nurses are going into travel nurse positions,” said Liedtke, who is also a family physician and OB-GYN. “They can sign big, big contracts…and that’s just not something we’re going to be able to match.”
Liedtke said it’s especially difficult to recruit nurses to work in the obstetrics unit of a rural hospital. At a larger facility, there might be different nurses dedicated to labor and delivery, the nursery, and postpartum care. But at Rolling Plains Memorial, one nurse has to handle all those roles.
Labor and delivery is a major investment for rural hospitals, requiring specialized nurses and a recommended 2-to-1 nurse-to-patient ratio during delivery. It’s rarely a money-making enterprise for these hospitals, particularly if they’re serving uninsured or Medicaid patients.
John Henderson, president of the Texas Organization of Rural and Community Hospitals, said struggling hospitals often see labor and delivery as an easy target for cuts. But he worries that these short-term closures and limited services will create a ripple effect that will ultimately leave rural hospitals worse off.
“You’ve compounded the problem by forcing people to leave the community when they need care,” he said.
If patients give birth at a hospital in a larger city, he worries they may be less likely to return to the local hospital for future medical care. “It won’t just be obstetrics,” he said. “They’ll probably end up seeing a pediatrician [at the larger hospital], and the next time they have a sprained ankle, that’s where they’re going.”
Transferring to larger hospitals
Many rural hospitals have already shaved down their services as much as possible, asking nurses to do double duty or transferring patients to larger hospitals for more specialized care.
Fewer than half of the state’s rural hospitals perform surgeries or have specialists such as cardiologists on staff, and many don’t have an intensive care unit. In normal times, it’s enough. But these days, there’s a logjam of patients who are waiting for a higher level of critical care than some of these hospitals can give on a long-term basis.
In the tiny Southeast Texas town of Anahuac, the local hospital is feeling the effects of soaring COVID-19 hospitalizations in Houston, an hour east.
“All of Houston’s medical center [complex of several hospitals] is in code red, meaning everyone is at capacity,” said William Kiefer, CEO of Chambers Health, which runs Anahuac’s hospital, OmniPoint Health. “And so the downstream effect of that is that we have two patients … who require transfer. We’ve had them for days. They’re not going anywhere.”
Rural hospitals say they can usually find beds in larger hospitals for patients who need to give birth, but even that’s become more tenuous as omicron and staffing shortages rage.
Teresa Baker, an OB/GYN with Texas Tech University Health Sciences Center in Amarillo, said she can always tell when there’s been an interruption in service somewhere else in the Panhandle. Suddenly patients are coming from farther away, later in the labor process, and often arriving via ambulance.
“We’re happy to take them,” Baker said. “The hospitals are doing a very selfless thing by shipping those patients, because they know they can’t handle them without the right staffing. The altruism is apparent.”
But hospitals in Amarillo are being walloped by the omicron variant just like everywhere else. During a recent shift, Baker said, seven out of 10 of their laboring patients were positive for COVID-19.
“We just assume everybody’s positive,” she said. “If the baby is born at full term and is healthy, then we can keep the mom and baby together, and the dad, because we can isolate them in the room.”
But many of the babies the hospital delivers have to go to the neonatal intensive care unit for additional care, which becomes much more difficult if the mother has tested positive for COVID-19.
“That’s what makes your heart bleed,” Baker said, “because these moms don’t even get to see their babies or nurse their babies because they’re positive. And it’s just a terrible situation.”
She said for the first time during the pandemic, the hospital has had to figure out issues like how to discharge babies from the NICU to COVID-positive parents.
“I said, what are they going to do, just meet her at the back door with her baby?” she recalls asking the nurse. “Because she can’t come into the hospital unless she absolutely needs to.”
Vaccine misinformation impacts staff, patients
Hospitals around the state are also contending with vaccine hesitancy among staff and patients. That’s just another challenge that’s hitting rural hospitals harder than better-resourced urban facilities.
For a time, Liedtke worried the labor and delivery unit at Rolling Plains Memorial might have to shut down, thanks to a federal vaccine mandate for health care workers that is tied up in the courts.
“To be very clear, I would love to see everyone vaccinated,” she said. “But from a staffing perspective, we were probably going to lose half of our [obstetrics] nurses.”
Other hospitals report similar concerns, saying they’re aware of large percentages of their nurses and hospital staff who would resign if they were required to get a vaccine.
OB/GYN doctors and nurses are also struggling to communicate vaccine information to their pregnant patients, many of whom are wary about a perceived lack of information about the effects of the vaccine on pregnancies.
“It’s so emotional for these moms, and I know they’re trying to make the best decision they can for their babies,” said Baker. “We just have to meet them where they are and just keep revisiting it.”
Baker said she tries to remind patients that the risks associated with getting very sick from COVID-19 outweigh any potential risks from the vaccine.
Holly Dunn, a maternal fetal medicine specialist in Abilene, has seen an uptick in patients needing specialized care because they develop COVID-19 symptoms during pregnancy.
“It’s more common now for my patients to have COVID or have had COVID than not,” she said.
She said it’s her unvaccinated patients who are developing serious pregnancy complications and fetal development issues, and even experiencing stillbirths. She’s implored her patients to get vaccinated for themselves and their children, and tells them about her own experience: She recently had a healthy baby after getting vaccinated.
“So I practice what I preach,” she said. “That gives me some street cred with my patients. If we can convince even one patient, it’s a victory.”
Karen Brooks Harper contributed to this report.
This story is reprinted from The Texas Tribune, a nonprofit, nonpartisan media organization that informs Texans—and engages with them—about public policy, politics, government, and statewide issues. The article originally appeared here.
CONTRIBUTOR